The Silent Crisis on Kerala’s Roads: Why We Need a "Low-Cost" Revolution in Trauma Training
The Silent Crisis on Kerala’s Roads: Why We Need a "Low-Cost" Revolution in Trauma Training
Every year, nearly 5,000 families in Kerala are shattered by road traffic fatalities. But the tragedy doesn’t end with the death toll. For every person lost, more than six others are left with life-altering permanent disabilities. This is not just a statistic; it is a public health emergency that demands a shift in how we approach the Golden Hour.
The Competency Gap in the Emergency Room
While India has made incredible strides with structured programs like Advanced Trauma Life Support (ATLS), we face a pragmatic hurdle: Accessibility and Cost. ATLS is the gold standard for a uniform trauma language, yet its high cost often prevents the very people at the frontlines—Interns, Junior Residents (JRs), and General Duty Medical Officers (GDMOs)—from getting certified. In the chaos of a poly-trauma case, enthusiasm isn't enough; we need skill-based, algorithmic muscle memory.
A Call for the "10 Basic Skills"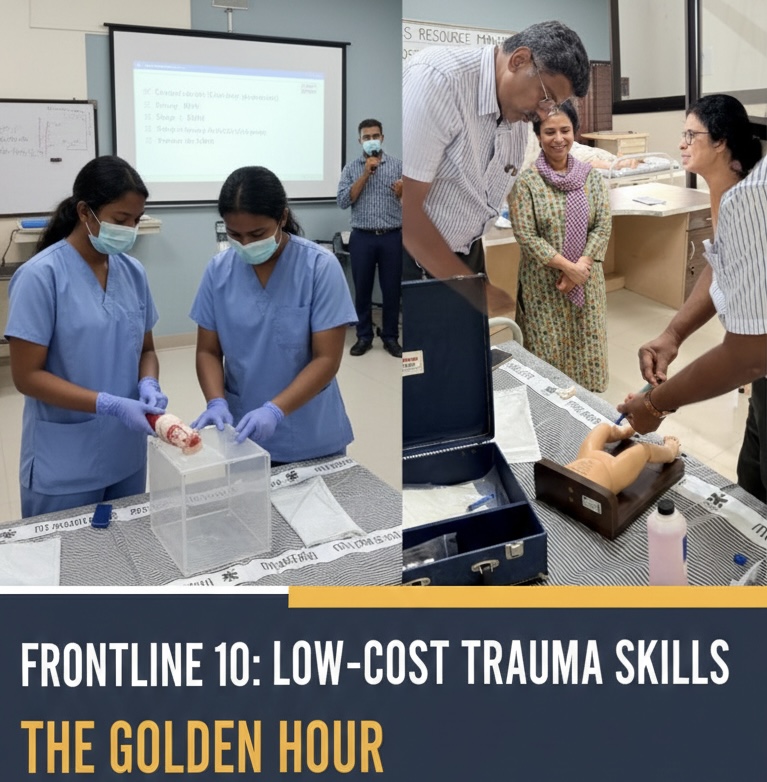
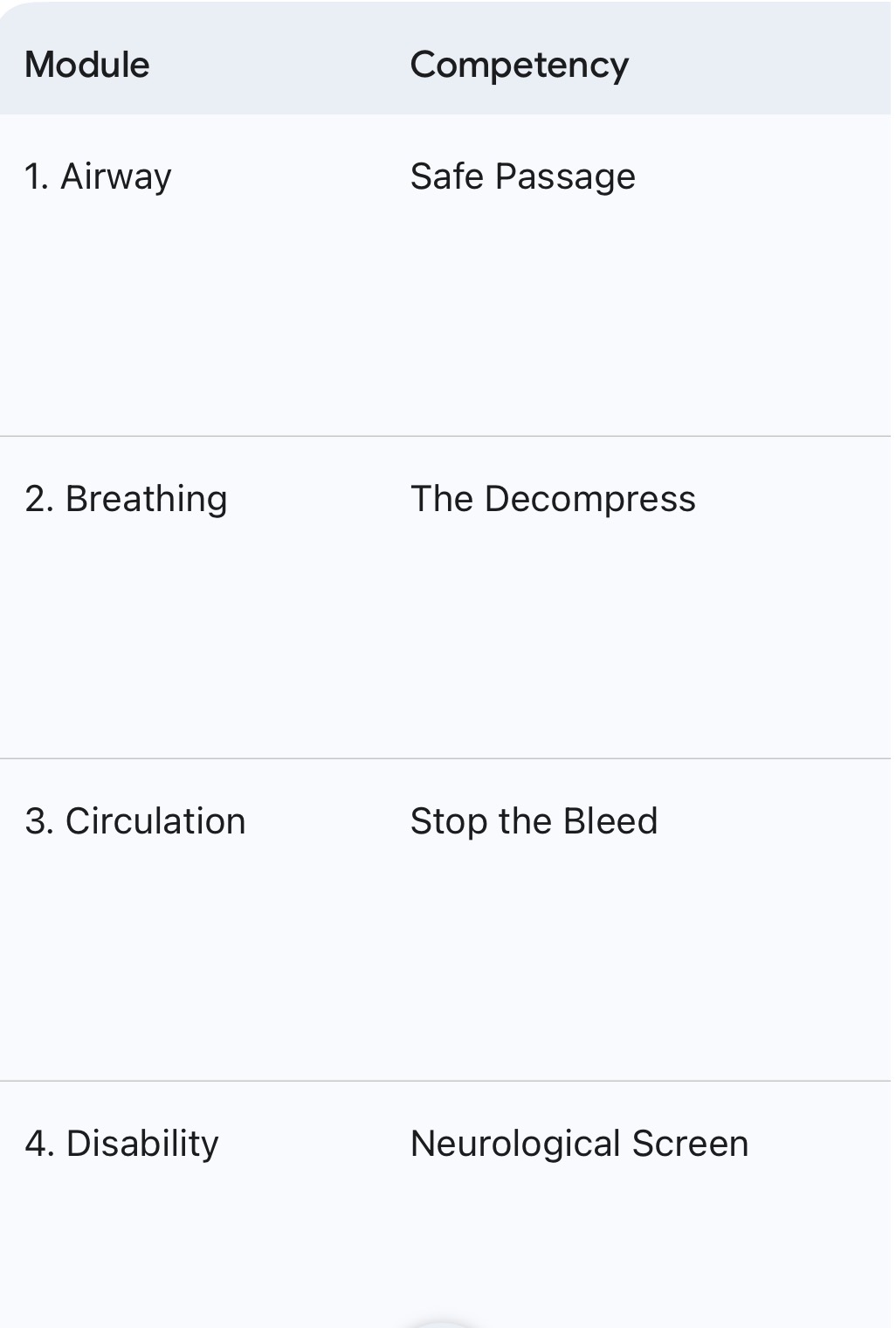
To bridge the gap between high-end certification and zero training, we must advocate for a low-cost, high-impact skill training model. We can save critical patients if every frontline doctor is proficient in these 10 core competencies:
1. Airway Management: Basic maneuvers and definitive airway.
2. Cervical Spine Protection: Proper immobilization techniques.
3. Needle Decompression: Identifying and relieving tension pneumothorax.
4. Intercostal Drain (ICD) Insertion: Managing hemothorax/pneumothorax.
5. Tourniquet & Pressure Packing: Aggressive external hemorrhage control.
6. Pelvic Binding: Stabilizing suspected pelvic fractures to prevent occult bleeding.
7. FAST Exam: Focused Assessment with Sonography for Trauma.
8. Splinting: Proper immobilization of long bone fractures.
9. Fluid Resuscitation: Balanced resuscitation and shock management.
10. Log Rolling & Secondary Survey: Ensuring no injury is missed during stabilization.
The Trauma Chain of Survival
Saving a life isn't a single event; it’s a chain. If one link fails, the patient loses. To reduce Kerala’s morbidity and mortality rates, we must strengthen every link in the Trauma Chain of Survival:
• Trauma Prevention: Education and stricter enforcement of road safety laws.
• Onsite Care: Bystander training and basic life support.
• En Route Care: Moving beyond "ambulance-as-a-taxi" to Critical Transport with trained paramedics.
• Advanced ER Care: Skill-based resuscitation by trained JRs and GDMOs.
• Destination Care: Rapid access to OTs, ICUs, and neurosurgical intervention.
• Rehabilitation: Returning the patient to a functional life.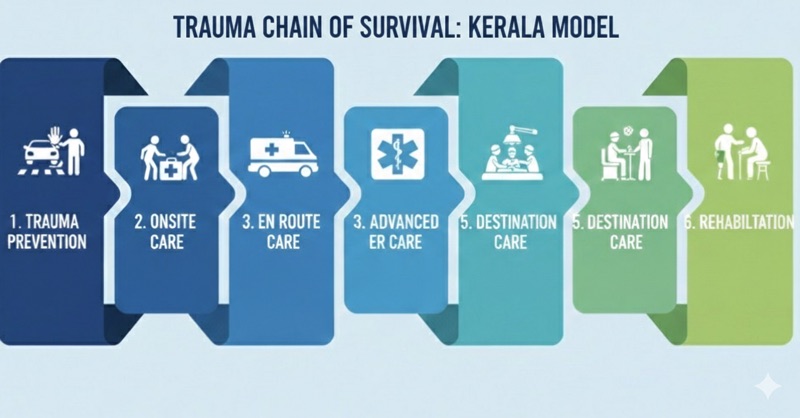
The Bottom Line
We don't just need more doctors; we need trauma-ready doctors. By democratizing trauma skills through low-cost, hands-on workshops, we can ensure that a patient’s survival doesn't depend on which hospital they reach, but on the competence of the first hands that touch them.
Let’s turn the "Golden Hour" into a "Hour of Certainty" for every citizen in Kerala.
#TraumaCare #KeralaHealth #MedicalEducation #RoadSafety #PublicHealth #ATLS #EmergencyMedicine #GoldenHour
Model for a low cost training
Part 1: The "Frontline 10" Training Syllabus
Objective: To transition Interns, JRs, and GDMOs from theoretical knowledge to procedural competence within a 1-day (8-hour) intensive workshop.
Part 2: The "Low-Cost" Simulation Lab (The DIY Kit)
You don’t need million-dollar mannequins to teach life-saving skills. Here is how to build a high-fidelity lab on a budget:
1. The "Chest Wall" (For ICD/Needle Decompression)
• Materials: A plastic crate or wooden frame covered with layers of foam (muscle), a layer of heavy-duty plastic (pleura), and a thick rubber sheet (skin).
• Cost-Saving: Use a simple bicycle inner tube filled with air under the "skin" to simulate the "hiss" of a tension pneumothorax when a needle is inserted.
2. The "Bleeding Limb" (For Tourniquets/Packing)
• Materials: PVC pipes padded with upholstery foam and covered in old leggings/denim.
• Realism: Use a hand-pumped sprayer filled with red-dyed water connected to a tube inside the foam to simulate arterial spurting.
3. The "Pelvic Simulator"
• Materials: Two plastic gallon jugs taped together to represent the iliac crests.
• Lesson: Teaches the "Inward and Downward" pressure technique and how to wrap a bedsheet binder tightly at the level of the greater trochanters.
4. FAST Exam Training
• Materials: Use a live volunteer (a student) and a basic portable ultrasound machine.
• Tip: If no ultrasound is available, use high-resolution printed "positive/negative" FAST images for a rapid-fire quiz to build visual recognition.